Digestive Health Institute
by Dr. Muffi
Digestive Health Institute
by Dr. Muffi
Life Expectancy After Total Hysterectomy
No, a total hysterectomy does not reduce life expectancy in most women.
Medical research shows that when the procedure is performed for appropriate conditions, women continue to live a normal lifespan. In many cases, overall health and quality of life improve after surgery.

What Is a Total Hysterectomy?
A total hysterectomy is a surgical procedure that involves removal of:
- Uterus
- Cervix
In some cases, it may also include:
- Ovaries
- Fallopian tubes
Types of Hysterectomy
- Total hysterectomy: Uterus + cervix removed
- Total hysterectomy with BSO: Uterus, cervix, ovaries, and tubes removed
- Subtotal hysterectomy: Uterus removed, cervix preserved
The presence or removal of ovaries is the most important factor influencing long-term health.
Scientific Evidence on Life Expectancy
- Studies show no increase in overall mortality in women undergoing hysterectomy after age 50
- Women under 45–50 may have a slightly higher cardiovascular risk only if ovaries are removed
- Hormone Replacement Therapy (HRT) significantly reduces these risks
Conclusion: Life expectancy remains normal in the vast majority of cases.
Life Expectancy Based on Ovary Removal
1. Without Ovary Removal
- Hormones remain stable
- Natural menopause occurs normally
- No increased long-term health risk
Life expectancy remains unchanged
2. With Ovary Removal (Early Menopause)
If ovaries are removed before natural menopause:
- Sudden drop in estrogen
- Early menopause
- Possible risks:
- Heart disease
- Osteoporosis
- Cognitive changes
With proper care (HRT, lifestyle, monitoring):
Life expectancy remains normal
Quick Comparison
| Scenario | Impact on Life Expectancy |
|---|---|
| Without ovary removal | No impact |
| With ovary removal + HRT | No significant impact |
| With ovary removal without HRT | Slight but manageable risk |
What Actually Affects Life Expectancy?
A hysterectomy itself is not the deciding factor. These matter more:
- Age at surgery
- Existing health conditions (diabetes, hypertension, obesity)
- Hormonal balance
- Lifestyle habits
- Regular follow-ups
Women who maintain good health practices often experience equal or better long-term outcomes.
Can Women Live a Normal Life After Hysterectomy?
Yes, most women lead completely normal, healthy lives.
Common benefits include:
- Relief from chronic pain
- Improved energy levels
- Better quality of life
- Emotional relief from ongoing symptoms
Emotional & Psychological Impact
It is normal to experience:
- Emotional adjustment
- Concerns about fertility
- Anxiety about long-term health
Support from healthcare professionals and counselling can significantly improve recovery and confidence.
Long-Term Health Considerations
Heart Health
- Regular exercise
- Blood pressure & cholesterol control
Bone Health
- Calcium and vitamin D
- Strength training
- Bone density checks if needed
Hormonal Balance
- Consider HRT if menopause occurs early
- Monitor symptoms like fatigue or hot flashes
How to Maintain a Long, Healthy Life After Hysterectomy
1. Stay Active
Walking, strength training, and yoga
2. Eat a Balanced Diet
Protein-rich, fiber-rich, and anti-inflammatory foods
3. Maintain a Healthy Weight
Excess weight can increase risks like heart disease and diabetes. Managing weight through lifestyle or medical guidance supports long-term health.
If obesity is a concern, structured medical weight management can play a role in improving overall outcomes.
4. Regular Health Checkups
- Breast screening
- Hormonal evaluation
- Metabolic health monitoring
Common Myths — Debunked
❌ Hysterectomy shortens life
✔ No scientific evidence supports this
❌ Women age faster after hysterectomy
✔ Aging depends on lifestyle and hormones, not the uterus
❌ Hormones completely stop
✔ Only if ovaries are removed — and manageable
When Can a Hysterectomy Be Life-Saving?
In conditions such as:
- Uterine or cervical cancer
- Severe bleeding
- Large fibroids
- Advanced endometriosis
The procedure can prevent complications and improve survival
Important Questions About Life After Hysterectomy
Does a full hysterectomy shorten your lifespan?
No. Studies show life expectancy remains normal.
How long can you live after a hysterectomy?
Women live a normal lifespan.
Does removing ovaries shorten life?
Only slightly affects risk if done early, but manageable.
Final Answer
Life expectancy after a total hysterectomy is normal.
With proper medical care, hormonal balance, and a healthy lifestyle, women can live long, active, and fulfilling lives.
FAQs: Life Expectancy After Total Hysterectomy?
Does a Total Hysterectomy Affect Life Expectancy?
A total hysterectomy does not reduce life expectancy for most women. Research shows that women who undergo hysterectomy generally live a normal lifespan, especially when the surgery is performed for non-cancerous conditions and proper post-operative care is followed.
- Can women live long after uterus removal?
Yes. The uterus is not essential for maintaining overall health after reproductive years. Once removed, it does not shorten lifespan or interfere with vital body functions. Most women continue to lead healthy, active lives following recovery. - Is hysterectomy safe in the long term?
Yes, a hysterectomy is considered safe in the long term. Outcomes are especially positive when the ovaries are preserved, as they continue to produce hormones that support bone, heart, and metabolic health. Even when ovaries are removed, appropriate hormone management can effectively maintain long-term well-being.
Can life expectancy decrease after hysterectomy at a young age?
Life expectancy does not decrease if a hysterectomy is performed at a young age, especially when the ovaries are preserved. If ovaries are removed early, proper hormone replacement therapy, regular follow-ups, and a healthy lifestyle help maintain a normal lifespan.
Do women age faster after a total hysterectomy?
No, women do not age faster after a total hysterectomy. Aging is influenced by genetics, lifestyle, and overall health — not uterus removal. When hormone balance is maintained, physical and mental aging progresses naturally and normally.
Overall, with regular medical follow-ups and a healthy lifestyle, a total hysterectomy does not negatively impact longevity or quality of life.
-
 Antral Gastritis Symptoms
Antral Gastritis Symptoms -
 Incisional Hernia Symptoms
Incisional Hernia Symptoms -
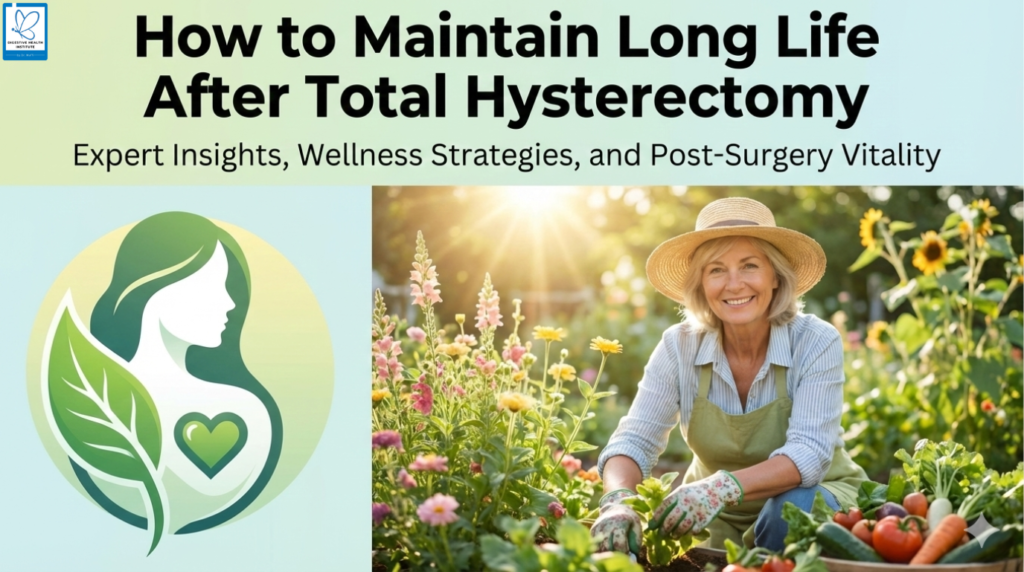
 Grade 1 Fatty Liver: Symptoms, Causes, Treatment, Diet & Recovery Guide
Grade 1 Fatty Liver: Symptoms, Causes, Treatment, Diet & Recovery Guide -
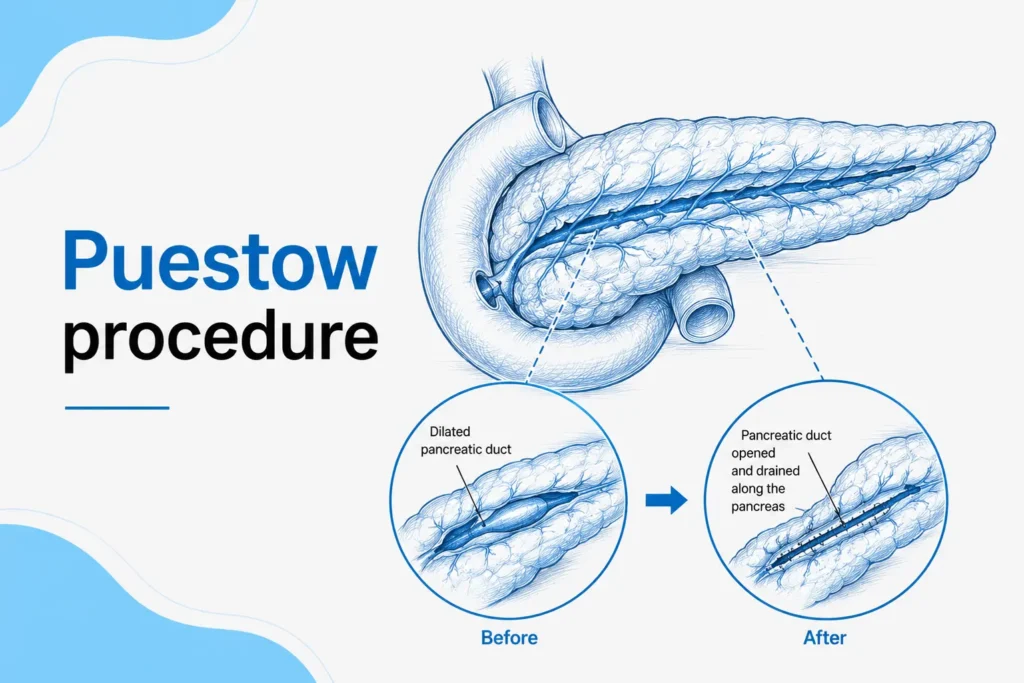 Puestow Procedure: Indications, Surgery, Recovery & Risks
Puestow Procedure: Indications, Surgery, Recovery & Risks -
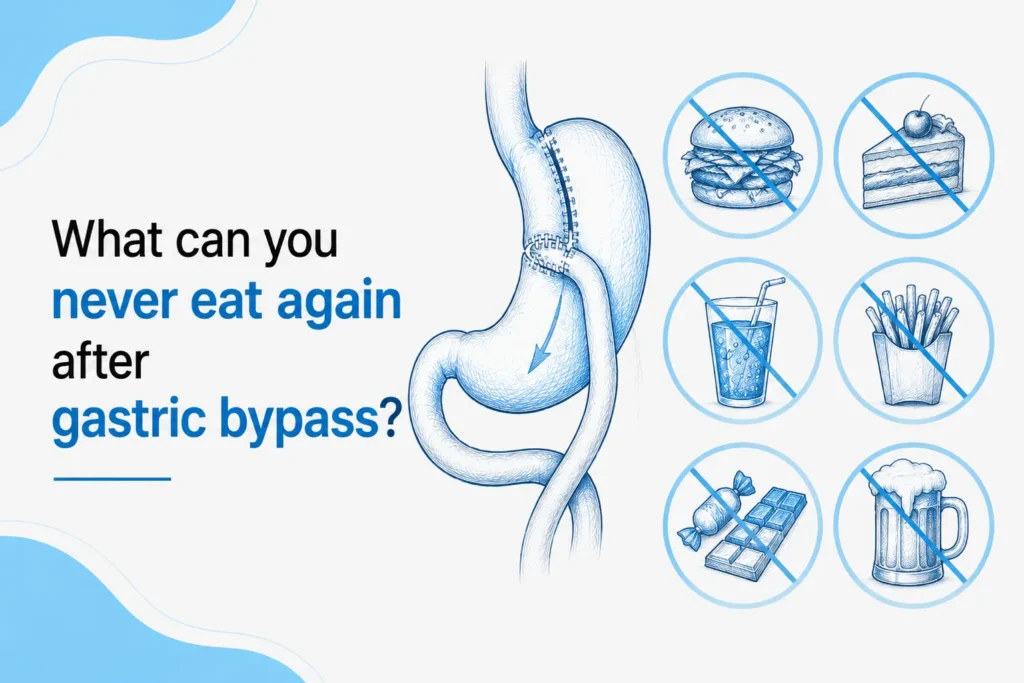 What can you never eat again after gastric bypass
What can you never eat again after gastric bypass -
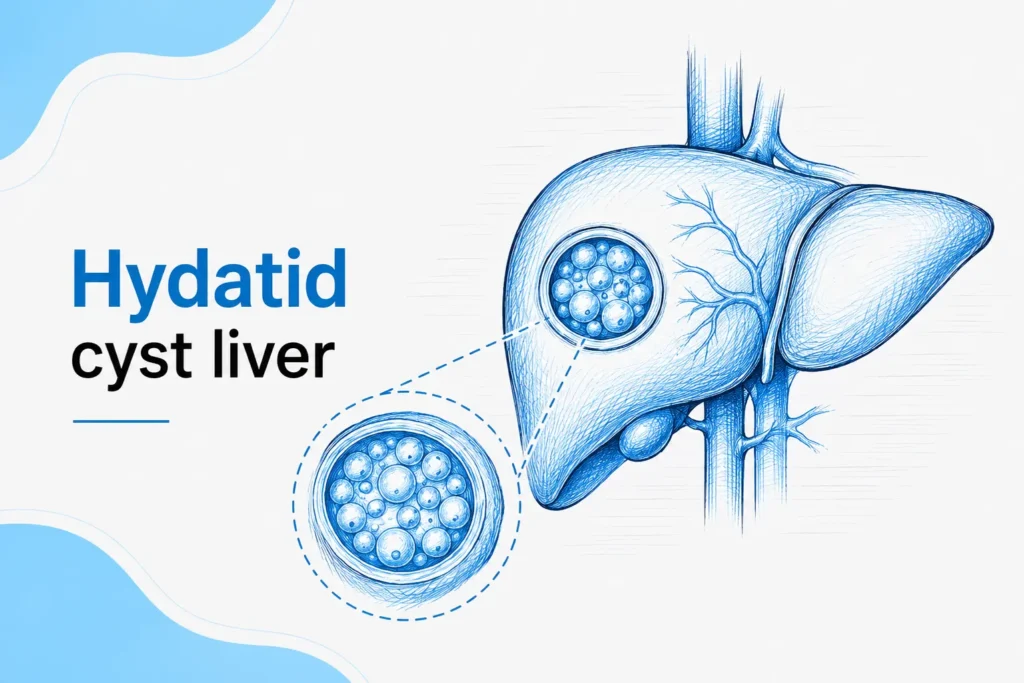 Hydatid Cyst Liver
Hydatid Cyst Liver -
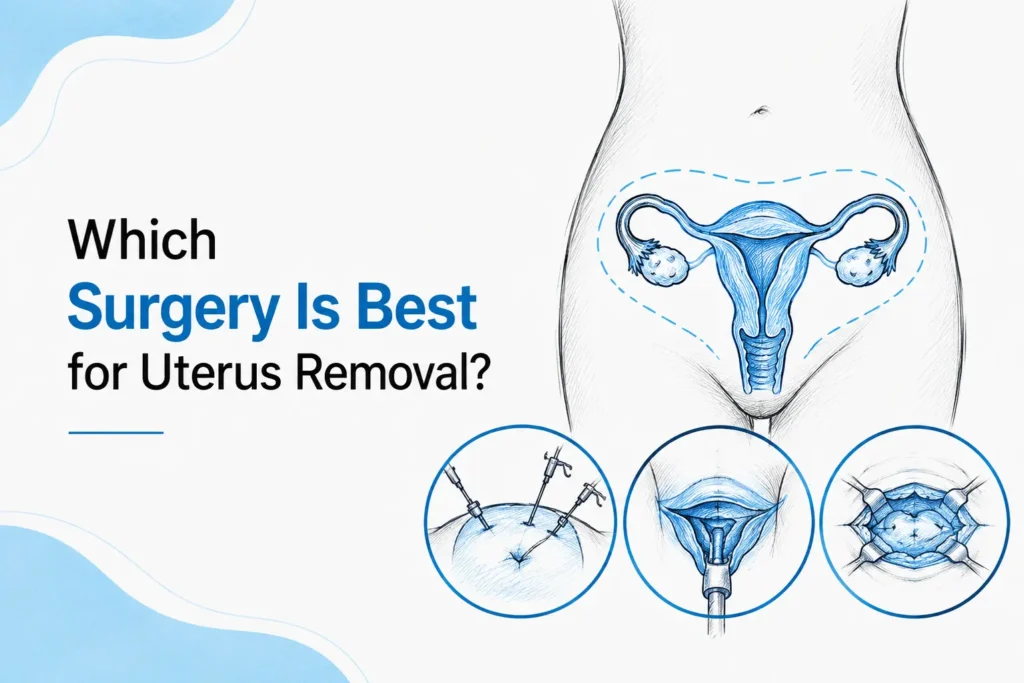 Which Surgery is best for Uterus Removal
Which Surgery is best for Uterus Removal -
 Is gallbladder wall thickening dangerous
Is gallbladder wall thickening dangerous